马дёҠжіЁеҶҢпјҢз»“дәӨжӣҙеӨҡеҘҪеҸӢпјҢдә«з”ЁжӣҙеӨҡеҠҹиғҪпјҢи®©дҪ иҪ»жқҫзҺ©иҪ¬зӨҫеҢәгҖӮ
жӮЁйңҖиҰҒ зҷ»еҪ• жүҚеҸҜд»ҘдёӢиҪҪжҲ–жҹҘзңӢпјҢжІЎжңүиҙҰеҸ·пјҹз«ӢеҚіжіЁеҶҢ
x
дёҖгҖҒfesoterodine йқһзҙўзҪ—е®ҡгҖҒfluspirilene ж°ҹж–Ҝеҝ…зҒөгҖҒposaconazole жіҠжІҷеә·е”‘гҖҒiloprost дјҠжҙӣеүҚеҲ—зҙ еҜ№ egfr зҡ„з»“еҗҲдәІе’ҢеҠӣи¶…иҝҮ йҳҝжі•жӣҝе°јпјӣеҜ№ her2 зҡ„ з»“еҗҲдәІе’ҢеҠӣи¶…иҝҮ жӢүеё•жӣҝе°ј
гҖҠA Holistic In silico Approach to Develop Novel Inhibitors Targeting ErbB1 and ErbB2 KinasesгҖӢиҝҷзҜҮи®әж–Үи®ІпјҢfesoterodine йқһзҙўзҪ—е®ҡгҖҒfluspirilene ж°ҹж–Ҝеҝ…зҒөгҖҒposaconazole жіҠжІҷеә·е”‘гҖҒiloprost дјҠжҙӣеүҚеҲ—зҙ иҝҷеҮ дёӘиҚҜпјҢеҜ№ egfr зҡ„з»“еҗҲдәІе’ҢеҠӣи¶…иҝҮ йҳҝжі•жӣҝе°јпјӣеҜ№ her2 зҡ„ з»“еҗҲдәІе’ҢеҠӣи¶…иҝҮ жӢүеё•жӣҝе°јгҖӮ
iloprost дјҠжҙӣеүҚеҲ—зҙ жҳҜжІ»з–—иӮәеҠЁи„үй«ҳеҺӢзҡ„иҚҜпјҢжң¬иә«е°ұжңүйӣҫеҢ–зҡ„еүӮеһӢпјҢиҝҷе°ұеҸҜд»ҘеҜ№иӮәйғЁз—…зҒ¶йӣҫеҢ–еұҖйғЁз»ҷиҚҜгҖӮ
fesoterodine йқһзҙўзҪ—е®ҡ жҳҜжІ»з–—иҶҖиғұиҝҮеәҰжҙ»еҠЁз—Үзҡ„пјҲе°ҝйў‘е°ҝжҖҘиҝҷдәӣй—®йўҳпјүпјҢгҖҠExposure to antimuscarinic medications for treatment of overactive bladder and risk of lung cancer and colon cancerгҖӢ иҝҷзҜҮж–Үз« и®ІдәҶз‘һе…ёзҡ„дёҖйЎ№еӣһйЎҫз ”з©¶пјҢз”Ё еҢ…жӢ¬йқһзҙўзҪ—е®ҡеңЁеҶ…зҡ„жІ»з–—иҶҖиғұиҝҮеәҰжҙ»еҠЁз—Үзҡ„жҠ—жҜ’и•ҲзўұиҚҜзү©зҡ„дәәпјҢжҜ”дёҚз”Ёзҡ„дәәпјҢеҫ—иӮ зҷҢе’ҢиӮәзҷҢзҡ„йЈҺйҷ©иҰҒе°ҸгҖӮ
жғіжғід№ҹиғҪзҗҶи§ЈпјҢиӮ зҷҢжІЎkrasгҖҒbrafзӘҒеҸҳзҡ„жІ»з–—ж–№жЎҲд№ӢдёҖе°ұжҳҜ жҠ—egfrжІ»з–—пјӣиӮәзҷҢжңүegfrдё»й©ұеҠЁеһӢзҡ„гҖӮ
дәҢгҖҒиҘҝзҪ—иҺ«еҸёжҠ—зҷҢзҡ„дёҙеәҠиҜ•йӘҢеүӮйҮҸ
дҫқз»ҙиҺ«еҸёжңүжҠ—зҷҢзҡ„ж ҮеҮҶеүӮйҮҸпјҢиҘҝзҪ—иҺ«еҸёжІЎжңүжҠ—зҷҢзҡ„ж ҮеҮҶеүӮйҮҸпјҢзӣ®еүҚиҜҙжҳҺд№ҰдёҠеҸӘжңүе…Қз–«жҠ‘еҲ¶зҡ„ж ҮеҮҶеүӮйҮҸгҖӮ
гҖҠSirolimus and trastuzumab combination therapy for HER2-positive metastatic breast cancer after progression on prior trastuzumab therapyгҖӢ
Constitutive activation of the PI3K/Akt/mTOR pathway has been suggested as a mechanism of resistance to trastuzumab therapy. This phase II trial was designed to evaluate the safety and clinical activity of daily oral sirolimus, a mammalian target of rapamycin (mTOR) inhibitor, in combination with trastuzumab in HER2-positive metastatic breast cancer following disease progression on prior trastuzumab therapy. Sirolimus 6 mg oral daily dose was administered with a standard dose and schedule of trastuzumab weekly or every 3 weeks. Pharmacodynamic studies included Western blot analysis of S6K1, phosphoS6K1, and mTOR in peripheral mononuclear cells, circulating tumor cells (CTC), and endothelial cells (CEC). Eleven patients were evaluable for safety; and nine were evaluable for response assessment. Subsequent enrollment was stopped due to slow accrual. Study treatment-related grade 3 toxicity included pneumonitis, myelosuppression (leukopenia/anemia), and dermatologic reactions (mucositis, nail changes and rash), with no grade 4 events. One patient received eight cycles (58 weeks) and achieved a partial response. Five patients treated for a total of 101 weeks (median 12 weeks, range 8-47 weeks) achieved stable disease as best response. Overall response rate was 1/9 (11 %) and clinical benefit rate was 4/9 (44 %). There was no statistically significant correlation between response and post-treatment change in levels of the mTOR pathway biomarkers, CTCs, HER2 CTCs, or CECs. Sirolimus 6 mg administered daily with trastuzumab appears to be well tolerated in patients with metastatic HER2-positive breast cancer following disease progression on prior trastuzumab therapy, with evidence of disease activity. mTOR inhibition may overcome resistance to trastuzumab in some HER2-positive tumors.
иҝҷдёӘдёҙеәҠиҜ•йӘҢйҮҢпјҢиҘҝзҪ—иҺ«еҸёжҳҜжҜҸеӨ©еҸЈжңҚ6жҜ«е…ӢиҒ”еҗҲжӣІеҰҘзҸ пјҢеҸҜд»ҘеҸӮиҖғиҝҷдёӘз”Ёжі•пјҢжҜҸеӨ©6жҜ«е…ӢгҖӮ
дёүгҖҒmasitinib 马иөӣжӣҝе°ј еҸҜд»ҘдҪңдёәmtorжҠ‘еҲ¶еүӮзҡ„жӣҝд»ЈиҚҜзү©
гҖҠBioinformatics and network-based screening and discovery of potential molecular targets and small molecular drugs for breast cancerгҖӢ
вҖңUsing BC cell lines, we validated that masitinib inhibits the mTOR signaling pathway and induces apoptotic cell death.вҖқ
иҝҷзҜҮи®әж–Үи®ІпјҢеҹәдәҺз”ҹзү©дҝЎжҒҜеӯҰе’ҢзҪ‘з»ңиҚҜзҗҶеӯҰпјҢзӯӣйҖүеҮәдәҶ masitinib 马иөӣжӣҝе°јпјҢеҸҜд»ҘдҪңдёәmtorжҠ‘еҲ¶еүӮзҡ„жӣҝд»ЈиҚҜзү©гҖӮ
马иөӣжӣҝе°јеҒҡиҝҮжҠ—зҷҢдёҙеәҠиҜ•йӘҢпјҢжңүдёҙеәҠеүӮйҮҸпјӣеҺҹж–ҷиҚҜд№ҹд№°еҫ—еҲ°пјҢжңүдёҖе®ҡзҡ„е®һз”ЁжҖ§гҖӮ
马иөӣжӣҝе°јеҲҶеӯҗйҮҸ498.64пјҢжҜ”дҫқз»ҙиҺ«еҸёгҖҒиҘҝзҪ—иҺ«еҸёе°ҸеӨҡдәҶгҖӮ
е®һйҷ…дёҠи®әеҜ№mtorзҡ„ic50еҖјпјҢдҫқз»ҙиҺ«еҸёгҖҒиҘҝзҪ—иҺ«еҸёеҖ’жҳҜеҫҲе°Ҹзҡ„пјҢе°Өе…¶иҘҝзҪ—иҺ«еҸёжңҖе°ҸпјҢзӣ®еүҚиҝҳжІЎзңӢеҲ°е“ӘдёӘиҚҜзү©жҜ”е®ғе°ҸгҖӮдҪҶдҫқз»ҙиҺ«еҸёгҖҒиҘҝзҪ—иҺ«еҸёзҡ„еҲҶеӯҗйҮҸйғҪиҰҒе…«д№қзҷҫпјҢе…Ҙи„‘е®һеңЁжҳҜеҫҲйҡҫгҖӮеҒҸеҒҸд№іи…әзҷҢи„‘иҪ¬з§»йңҖиҰҒз”ЁеҲ° mtorиҚҜзҡ„зӘҒеҸҳжү©еўһжңҖеӨҡгҖӮ
иҰҒжүҫеҲ°еҗҲйҖӮиғҪз”Ёзҡ„mtorжҠ‘еҲ¶еүӮжӣҝд»ЈиҚҜзү©йқһеёёеӣ°йҡҫпјҢжҲ‘зҝ»дәҶ200еӨҡзҜҮиӢұж–Үи®әж–Үд№ҹе°ұжүҚжүҫеҲ° 马иөӣжӣҝе°јиҝҷдёӘзңӢдёҠеҺ»еҘҪеғҸиҝҳиғҪз”ЁдёҖз”ЁпјҢе…¶д»–зҡ„жҖ»жҳҜжңүиҝҷж ·йӮЈж ·зҡ„й—®йўҳгҖӮ
жҜ”еҰӮгҖҠLomitapide, a cholesterol-lowering drug, is an anticancer agent that induces autophagic cell death via inhibiting mTORгҖӢ иҝҷзҜҮи®әж–Үи®ІеҲ°пјҢLomitapide жҙӣзҫҺд»–жҙҫпјҢдёҖз§ҚжІ»з–—й«ҳиғҶеӣәйҶҮиЎҖз—Үзҡ„иҚҜпјҢжңүеҫҲеҘҪзҡ„жҠ‘еҲ¶mtorзҡ„дҪңз”ЁгҖӮиҖҢдё”жҜ”дҫқз»ҙиҺ«еҸёгҖҒиҘҝзҪ—иҺ«еҸёеҘҪпјҢеӣ дёә elF4E иЎЁиҫҫй«ҳзҡ„иҜқпјҢдҫқз»ҙиҺ«еҸёгҖҒиҘҝзҪ—иҺ«еҸёиҝҷдәӣиҚҜе°ұе®№жҳ“иҖҗиҚҜпјҢиҖҢ elF4E иЎЁиҫҫй«ҳ еҜ№ жҙӣзҫҺд»–жҙҫеҪұе“ҚдёҚеӨ§гҖӮ
зңӢдёҠеҺ»еҫҲеҘҪпјҢдҪҶжҳҜд»”з»ҶдёҖз ”з©¶еүӮйҮҸпјҢе°ұжңүеӨ§й—®йўҳдәҶпјҡи®әж–ҮйҮҢзҡ„еҠЁзү©жЁЎеһӢеүӮйҮҸжҚўз®—жҲҗдәәдҪ“еүӮйҮҸпјҢеӨ§жҰӮиҰҒжҜҸеӨ©жҜҸе…¬ж–Ө2жҜ«е…Ӣе·ҰеҸіпјҢдёҖдёӘ50е…¬ж–Өзҡ„жӮЈиҖ…жҜҸеӨ©иҰҒеҗғ100жҜ«е…ӢгҖӮиҝҷиғҪдёҚиғҪеҗғпјҢиғҪдёҚиғҪиҖҗеҸ—е°ұдёҚзҹҘйҒ“дәҶгҖӮеҸҰеӨ–жҙӣзҫҺд»–жҙҫзҡ„еҲҶеӯҗйҮҸд№ҹиҰҒиҫҫеҲ°693.72дәҶпјҢеҫҲеӨ§дәҶпјҢе…Ҙи„‘зңӢдёҠеҺ»д№ҹжҢәйҡҫзҡ„ж ·еӯҗгҖӮ
еӣӣгҖҒдёӘдҪ“зІҫеҮҶжІ»з–—зҡ„еҸ‘еұ•ж–№еҗ‘
гҖҠDrug repurposing using transcriptome sequencing and virtual drug screening in a patient with glioblastomaгҖӢ
иҝҷзҜҮи®әж–Үи®Ізҡ„дёҖдёӘзІҫеҮҶжІ»з–—зҡ„з—…дҫӢпјҢйҮҮз”Ёзҡ„зӯӣйҖүжңҖе…·дёӘдҪ“еҢ–зү№зӮ№зҡ„ж–№жЎҲпјҢжҲ‘ж„ҹи§үиҝҷз§Қж–№жі•жҳҜзІҫеҮҶжІ»з–—зҡ„еҸ‘еұ•ж–№еҗ‘гҖӮ
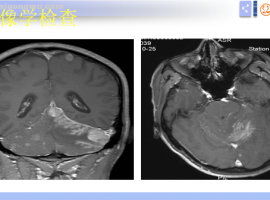
дёҖдҪҚи„‘иғ¶иҙЁзҳӨзҡ„жӮЈиҖ…пјҢе…ҲеҒҡе…ЁеҘ—еҹәеӣ жЈҖжөӢпјҢжөӢеҮәжқҘBRAF (47-438del) е’Ң PIK3R1 (G376R) зӯүзӘҒеҸҳгҖӮеӣ дёәдёҚжҳҜ braf V600E иҝҷз§Қеёёи§ҒзғӯзӮ№зӘҒеҸҳпјҢжүҖд»ҘжІЎжңүйҮҮ用常规зҡ„braf зҡ„йқ¶еҗ‘иҚҜж–№жЎҲпјҢиҖҢжҳҜжӢҝиҝҷдәӣе…ій”®зӘҒеҸҳзҡ„жҷ¶дҪ“з»“жһ„пјҢеҺ»и·ҹFDAе·Із»Ҹжү№еҮҶдёҠеёӮзҡ„иҚҜзү©пјҲдёҚйҷҗдәҺжҠ—зҷҢиҚҜзү©пјүпјҢиҝӣиЎҢеҲҶеӯҗеҜ№жҺҘпјҢи®Ўз®—з»“еҗҲдәІе’ҢеҠӣгҖӮзӯӣйҖүеҮәз»“еҗҲдәІе’ҢеҠӣжңҖй«ҳзҡ„10з§ҚиҚҜзү©пјҢеҶҚеңЁ10з§ҚиҚҜзү©йҮҢзӯӣйҖү иғҪз©ҝи¶ҠиЎҖи„‘еұҸйҡңгҖҒжҜ’еүҜдҪңз”Ёе°ҸгҖҒеҸҜеҸҠжҖ§ејәзҡ„иҚҜзү©пјҢжңҖз»ҲйҖүе®ҡдәҶдёӨдёӘи’ҪзҺҜзұ»еҢ–з–—иҚҜзҡ„и„ӮиҙЁдҪ“еүӮеһӢгҖӮ
иҝҷе®Ңе…ЁжҳҜйҮҸиә«е®ҡеҒҡзҡ„дёӘдҪ“еҢ–зІҫеҮҶеҢ–зҡ„жІ»з–—ж–№жЎҲпјҢиҝҷз§Қж–№жі•зӣ®еүҚе®һзҺ°жҠҖжңҜдёҠеә”иҜҘдёҚжҳҜеҫҲйҡҫпјҢеӣ дёәжҷ¶дҪ“ж•°жҚ®еә“гҖҒиҚҜзү©ж•°жҚ®еә“гҖҒи®Ўз®—з»“еҗҲдәІе’ҢеҠӣзҡ„иҪҜ件д№Ӣзұ»зҡ„пјҢйғҪжҳҜзҺ°жҲҗзҡ„гҖӮе°ұз®—е‘Ҫзү№еҲ«дёҚеҘҪпјҢзӘҒеҸҳзҡ„зӮ№зҡ„йӮЈдёӘжҷ¶дҪ“з»“жһ„ж•°жҚ®еә“йҮҢжІЎжңүпјҢд№ҹжҳҜеҸҜд»Ҙи®©дәәдё“й—ЁиҝӣиЎҢеҲҶжһҗзҡ„гҖӮ
дә”гҖҒгҖҠжҢҮеҚ—гҖӢгҖҒиҜўиҜҒзҡ„ж №жң¬й—®йўҳ
жҠҠгҖҠжҢҮеҚ—гҖӢзҡ„жүҖдҫқжҚ®зҡ„еҫӘиҜҒиҜҒжҚ®пјҢеҪ“жҲҗеҲ¶е®ҡз”ЁиҚҜж–№жЎҲзҡ„йҮ‘科зҺүеҫӢпјҢжңҖж №жң¬жңҖж ёеҝғзҡ„й—®йўҳпјҢжҳҜжӢҝзҫӨдҪ“ж•°жҚ®зӣҙжҺҘзӯүеҗҢдәҺдёӘдҪ“з–—ж•ҲгҖӮ
жүҖи°“еҫӘиҜҒиҜҒжҚ®зҡ„йӮЈдәӣдёҙеәҠиҜ•йӘҢз»“жһңпјҢжІЎжңүе“ӘдёӘдёҙеәҠиҜ•йӘҢжҳҜе…Ҙз»„жӮЈиҖ…дёӘдёӘйғҪжңүж•Ҳзҡ„пјӣиҖҢдё”е°ұз®—еңЁжңүж•Ҳзҡ„йӮЈдәӣжӮЈиҖ…йҮҢпјҢд№ҹеҲҶз–—ж•ҲеҘҪдёҺз–—ж•ҲдёҖиҲ¬гҖӮ
еҸӮеҠ йӮЈдёӘдёҙеәҠиҜ•йӘҢзҡ„йӮЈзҫӨдәәйҮҢзҡ„дёҖйғЁеҲҶдәәжңүж•ҲпјҢжҳҜжҖҺд№Ҳе°ұеҸҜд»Ҙеӣ жӯӨйў„еҲӨйў„жөӢдҪ д№ҹдјҡжңүж•Ҳзҡ„пјҹиҝҷдёӘй—®йўҳпјҢе°ұжҳҜиҰҒе®іжүҖеңЁгҖӮ
|



 иҝҷжҳҜиҖҗиҚҜдәҶеҗ—пјҹ
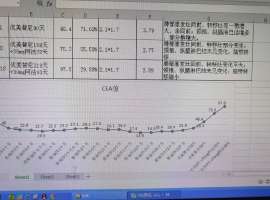
2024е№ҙ8жңҲд»ҪзЎ®иҜҠиӮәи…әзҷҢеӣӣжңҹпјҢејҖе§ӢеҚЎй“Ӯ+еҹ№зҫҺжӣІеЎһ+зү№з‘һжҷ®еҲ©жІ»з–—6ж¬ЎпјҢжңҹй—ҙжҜҸдёӨж¬ЎжІ»з–—еҗҺеӨҚ
иҝҷжҳҜиҖҗиҚҜдәҶеҗ—пјҹ
2024е№ҙ8жңҲд»ҪзЎ®иҜҠиӮәи…әзҷҢеӣӣжңҹпјҢејҖе§ӢеҚЎй“Ӯ+еҹ№зҫҺжӣІеЎһ+зү№з‘һжҷ®еҲ©жІ»з–—6ж¬ЎпјҢжңҹй—ҙжҜҸдёӨж¬ЎжІ»з–—еҗҺеӨҚ
 ж°ҙиӮҝпјҹе‘•еҗҗпјҹиӮқиӮҫеҠҹиғҪејӮеёёпјҹдёҖж–ҮиҜ»жҮӮ
дҪңиҖ…пјҡйӣЁиҝҮеӨ©жҷҙ
еҰӮд»ҠпјҢиӮәзҷҢжІ»з–—йўҶеҹҹзҡ„еҘҪж¶ҲжҒҜи¶ҠжқҘи¶ҠеӨҡгҖӮе°Өе…¶жҳҜй’ҲеҜ№зү№е®ҡеҹәеӣ еҸҳејӮзҡ„йқ¶еҗ‘
ж°ҙиӮҝпјҹе‘•еҗҗпјҹиӮқиӮҫеҠҹиғҪејӮеёёпјҹдёҖж–ҮиҜ»жҮӮ
дҪңиҖ…пјҡйӣЁиҝҮеӨ©жҷҙ
еҰӮд»ҠпјҢиӮәзҷҢжІ»з–—йўҶеҹҹзҡ„еҘҪж¶ҲжҒҜи¶ҠжқҘи¶ҠеӨҡгҖӮе°Өе…¶жҳҜй’ҲеҜ№зү№е®ҡеҹәеӣ еҸҳејӮзҡ„йқ¶еҗ‘
 еҘҘиҘҝиҖҗиҚҜжҚўдјҸзҫҺдёүдёӘжңҲиҖҗиҚҜпјҢжұӮеҗҺз»ӯжІ»
жҜҚдәІпјҢеҲҡж»Ў69еІҒпјҢ2021е№ҙ1жңҲеә•зЎ®иҜҠиӮәи…әзҷҢеӣӣжңҹпјҢеҸҢиӮәгҖҒеҸҢдҫ§иғёиҶңиҪ¬з§»пјҢL858R 21зӘҒеҸҳпјҢзӣ®
еҘҘиҘҝиҖҗиҚҜжҚўдјҸзҫҺдёүдёӘжңҲиҖҗиҚҜпјҢжұӮеҗҺз»ӯжІ»
жҜҚдәІпјҢеҲҡж»Ў69еІҒпјҢ2021е№ҙ1жңҲеә•зЎ®иҜҠиӮәи…әзҷҢеӣӣжңҹпјҢеҸҢиӮәгҖҒеҸҢдҫ§иғёиҶңиҪ¬з§»пјҢL858R 21зӘҒеҸҳпјҢзӣ®
 и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§» дёӯдҪҚжІ»з–—з”ҹеӯҳжңҹ 3-6жңҲ
и„‘иҶңиҪ¬з§»зҡ„дёҙеәҠиЎЁзҺ°
и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§» дёӯдҪҚжІ»з–—з”ҹеӯҳжңҹ 3-6жңҲ
и„‘иҶңиҪ¬з§»зҡ„дёҙеәҠиЎЁзҺ°
 ејҹејҹиӮәзҷҢжҷҡжңҹеҚ•йқ¶еҗ‘иҚҜжІ»з–—8е№ҙжІЎиҖҗиҚҜ
и®Іиҝ°иҖ…пјҡеӨ©еӨ©ж¬ўд№җж•ҙзҗҶиҖ…пјҡpearжҲ‘们дёҖ家жҳҜе…ёеһӢзҡ„зҷҢз—Ү家ж—ҸеҸІе®¶еәӯпјҢжҲ‘е’ҢеҰ№еҰ№ж—©е№ҙй—ҙйғҪжҹҘеҮә
ејҹејҹиӮәзҷҢжҷҡжңҹеҚ•йқ¶еҗ‘иҚҜжІ»з–—8е№ҙжІЎиҖҗиҚҜ
и®Іиҝ°иҖ…пјҡеӨ©еӨ©ж¬ўд№җж•ҙзҗҶиҖ…пјҡpearжҲ‘们дёҖ家жҳҜе…ёеһӢзҡ„зҷҢз—Ү家ж—ҸеҸІе®¶еәӯпјҢжҲ‘е’ҢеҰ№еҰ№ж—©е№ҙй—ҙйғҪжҹҘеҮә


 жҸҗеҚҮеҚЎ
жҸҗеҚҮеҚЎ зҪ®йЎ¶еҚЎ
зҪ®йЎ¶еҚЎ жІүй»ҳеҚЎ
жІүй»ҳеҚЎ е–§еҡЈеҚЎ
е–§еҡЈеҚЎ еҸҳиүІеҚЎ
еҸҳиүІеҚЎ еҚғж–ӨйЎ¶
еҚғж–ӨйЎ¶ жҳҫиә«еҚЎ
жҳҫиә«еҚЎ